%402x.d65c0b0b.webp)

Uveal melanoma diagnosis: Key insights for early detection
Uveal melanoma manifests itself in many ways. Some people may experience blurred vision, floaters, flashing lights and shadow in the vision. For many others, however, there is no sign of irregular vision, and the tumor may go undetected until it is found during a routine dilated eye exam.
To check for abnormalities and make a diagnosis, the doctor uses an indirect ophthalmoscope to examine the back part of the inside of the eye. Your doctor may also use ultrasound, fundus photography, fluorescein angiography, or even a biopsy, to establish the diagnosis. However, uveal melanoma is one of the few cancers that can be accurately diagnosed without a biopsy in most cases.
Common symptoms of Uveal Melanoma

Will your eye cancer spread to other parts of your body?
For uveal melanoma patients and their loved ones, one of the big questions is whether the eye cancer will spread, or metastasize, to other parts of the body. While your healthcare provider will explain that there is approximately a 50% chance that it will not, you need to decide if you'd like to know the answer with far more precision.
The understanding has been that large tumors typically are at higher risk, and smaller tumor size is predictive of better survival. However, that is not always the case. In recent years, prognostic tests have been developed to more accurately assess a uveal melanoma tumor’s biology and likelihood of spreading.


Several factors have been historically associated with higher risk of metastasis including large tumor size, location, orange pigment overlying the tumor and older age. However, multiple published studies have found that the DecisionDx-UM test result is the most accurate and clinically impactful risk factor.
Now you can learn your risk of metastasis with precision
DecisionDx-UM, the most widely used prognostic test in the U.S., makes it possible to learn your prognosis with the highest degree of accuracy available. The test predicts rates of distant metastasis, or spreading, over five years, the period for which scientific data has been collected. This information can be incredibly valuable in helping you and your doctor determine your management plan. Many patients report other benefits as well: Some say knowing the likely course of their disease makes it easier to cope. Others say it helps them make important life-planning decisions. In a study of 177 uveal melanoma patients, 99% of patients reported gaining value from their DecisionDx-UM test result, regardless of their tumor class.

With a 2% risk of spreading over the next five years

With a 21% risk of spreading over the next five years

With a 72% risk of spreading over the next five years
Healthcare providers use DecisionDx-UM to predict metastasis and guide follow-up care
We know that as many as half of uveal melanomas have metastasized by the time the eye tumor is discovered and treated. However, the cancer cells are so tiny that they go undetected by today’s imaging techniques—an event known as micrometastasis. Most ocular oncologists use a prognostic test called DecisionDx-UM to determine the likelihood that the cancer will metastasize (spread). Multiple recent studies have shown that this test is being used to match a patient’s risk to an appropriate surveillance plan.
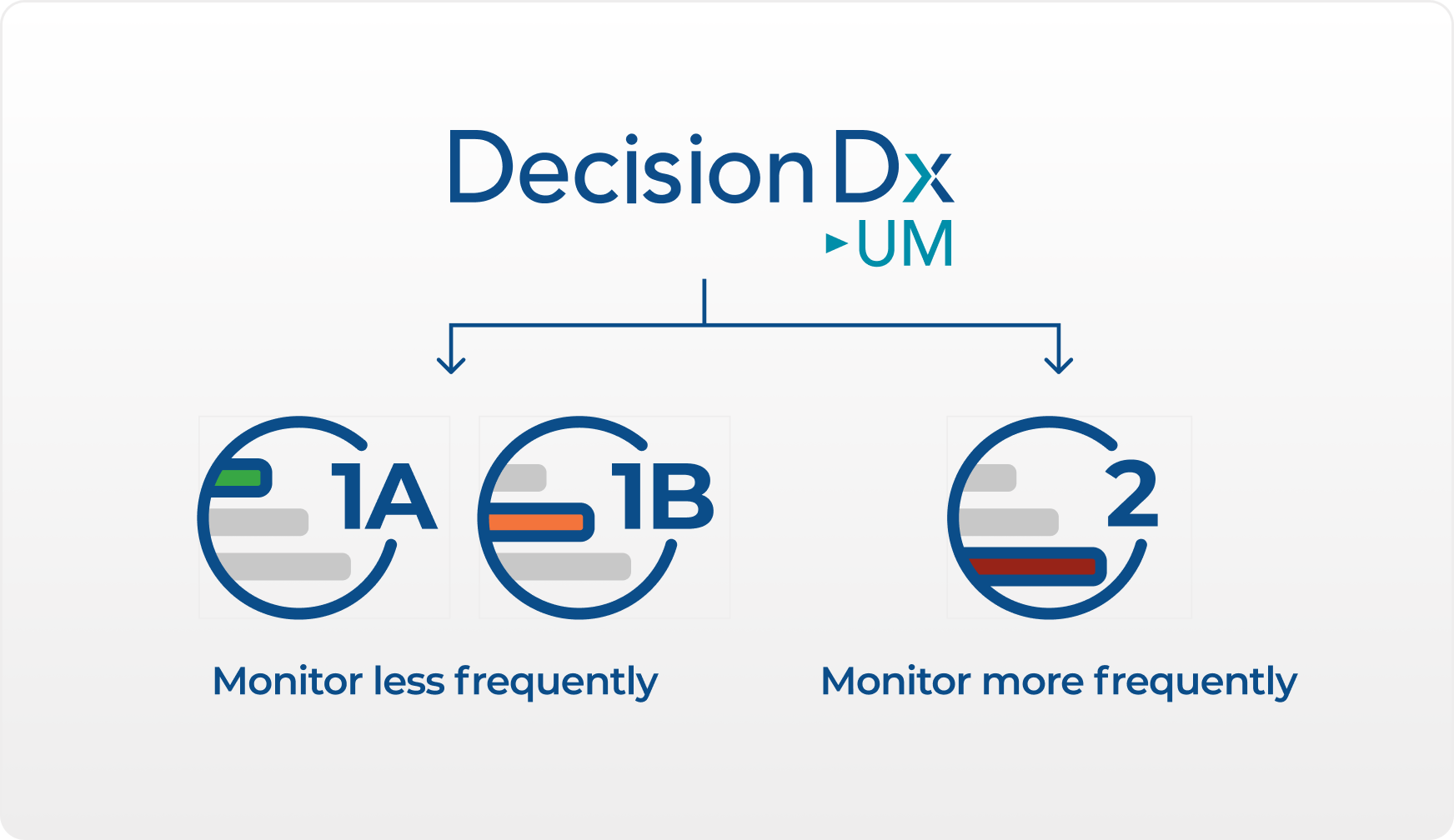
For instance, according to these studies, if the tumor was identified as being at low (Class 1A) or intermediate (Class 1B) risk of metastasis, doctors recommended a low intensity surveillance program such as alternating between periodic liver function tests and ultrasound or MRI. If the tumor was at a high risk (Class 2), the doctors monitored for metastasis more frequently and used more advanced imaging such as ultrasound, MRI, or CT scans, along with liver function tests.
If your doctor catches the spread (or metastasis) of your eye melanoma early or when it is still small, there are interventions that may be considered, including laparascopic radioablation, hepatic arterial perfusion chemoembolization, and surgical resection (removal).
The hope is that intensive monitoring for metastasis may lead to early detection and treatment that could produce better outcomes for patients. Along these lines, there are clinical trials for patients whose eye melanoma is expected to spread based on their DecisionDx-UM result. This early treatment to prevent spread of the tumor is called adjuvant therapy. As always, decisions regarding the risk and benefits of specific surveillance and treatment plans are better decided between a patient and their physician.
