Case Study

High-risk melanoma diagnosed and risk-stratified with MyPath Melanoma and DecisionDx-Melanoma
A 74-year-old male with a dome-shaped red papule on right central frontal scalp.
Case details

A 74-year-old man presents with a dome-shaped red papule on right central frontal scalp. A shave biopsy was collected. Clinical impression was to rule out basal cell carcinoma.


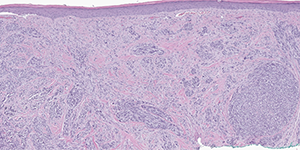
The following atypical findings were noted from the H&E:
- Asymmetric, intradermal melanocytic lesion with spindled and epithelioid melanocytes
- Small variably sized nests in superficial dermis with larger component of melanocytes within a fibrotic stroma
- Melanocytes have abundant cytoplasm, large nuclei, and some are irregularly pigmented
- Lesion extends to the deep and peripheral margins
- MelanA and SOX-10 were also used to examine the lesion. Both stains were positive.
- Further straining was used to assess the malignant potential. While positive PRAME staining and Ki-67 proliferation index of 10% were both consistent with malignancy, p16 was completely retained.

Following an extensive histopathological work-up, the differential diagnosis still could not exclude melanoma due to the unusual finding of retained p16 and the lack of an epidermal component. MyPath Melanoma was ordered by the dermatopathologist to clarify the malignant potential of the lesion.
MyPath Melanoma gene expression profile resulted in a score of 0.8 which is suggestive of a malignant neoplasm.
Malignant Melanoma, Stage pT2a
- Breslow depth: 1.5 mm, AT LEAST
- Mitotic rate: <1/mm2
- Ulceration: Not present
- Margins involved: deep and lateral
- Histologic type: spindled
- TILs: Minimal
- Regression: Absent
- Microsatellites: Not identified
With a transected base, the true depth and stage of the lesion was unknown. The dermatologist requested DecisionDx-Melanoma to determine the patient’s individual risk of recurrence and likelihood for a positive sentinel lymph node biopsy.

Class 2A - Increased risk
- i31-ROR: MSS: 91.9% | DMFS: 86.4% | RFS: 78.8%
- i31-SLNB: 9.3%
Due to the Class 2A score, the patient was referred to surgical oncology and underwent a wide-local excision and sentinel lymph node biopsy which was negative. BRAF testing was performed and as negative.
Patient is being followed closely by the dermatologist and had a clear lymph node examination at 6-month follow-up.